LessonPediatric Considerations in Chest Trauma
Pediatric Considerations in Chest Trauma
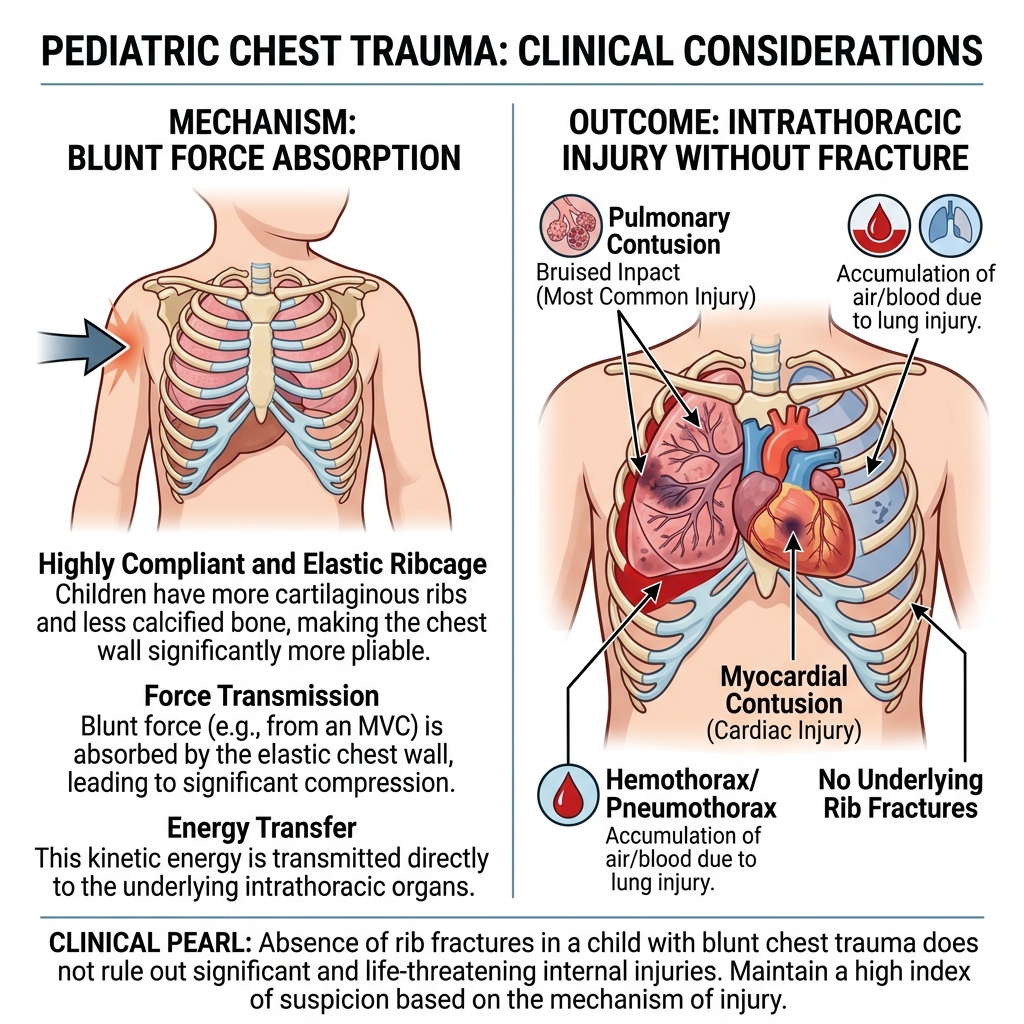
Children present differently than adults in chest trauma due to anatomical and physiological differences, especially increased chest wall flexibility (compliance). This flexibility allows significant internal injury without obvious external damage.
Key Anatomical Differences
- Pediatric ribs are more elastic and less calcified
- The chest wall absorbs force instead of fracturing
Clinical Impact
Higher risk of: Intrathoracic injury without rib fractures, Traumatic asphyxia, Commotio cordis. Serious internal injury may exist despite a normal-looking chest wall.
Physiological Differences
Mediastinal Mobility
Structures in the chest shift more easily. Even small pneumothorax/hemothorax can compress the heart and reduce venous return, causing rapid progression to tension physiology.
Higher Metabolic Demand
Increased oxygen requirements relative to body size. Greater cardiopulmonary reserve. Children may appear stable initially but can deteriorate suddenly and rapidly.
Red Flags for Abuse
Be vigilant for signs of non-accidental trauma in pediatric chest injuries:
- Injuries inconsistent with history
- Multiple injuries at different stages
- Delayed medical care
- Rib fractures in very young children, Skull fractures, Eye findings (hyphema), Implausible mechanical explanations.
Assessment and Management
Airway & Breathing
Watch for secretions, airway swelling, or signs of bronchial injury. Prepare for airway compromise early. Monitor SpO₂ and ETCO₂. Provide oxygen and PEEP if ventilatory support is required.
Circulation
Assess for shock, cardiac involvement, or mediastinal shift effects. Provide IV access and fluid resuscitation (up to ~20 mL/kg). Maintain suspicion for tamponade.
Disability
Assess mental status (AVPU/GCS). Mental status changes may occur before vital sign changes.
Key Takeaway
- Pediatric chest trauma can be deceptively severe.
- Significant internal injury may exist with minimal external findings.
- Children may appear stable, then rapidly decompensate.
- Always maintain a high index of suspicion and reassess frequently.