LessonNeonatal bradycardia
Neonatal bradycardia
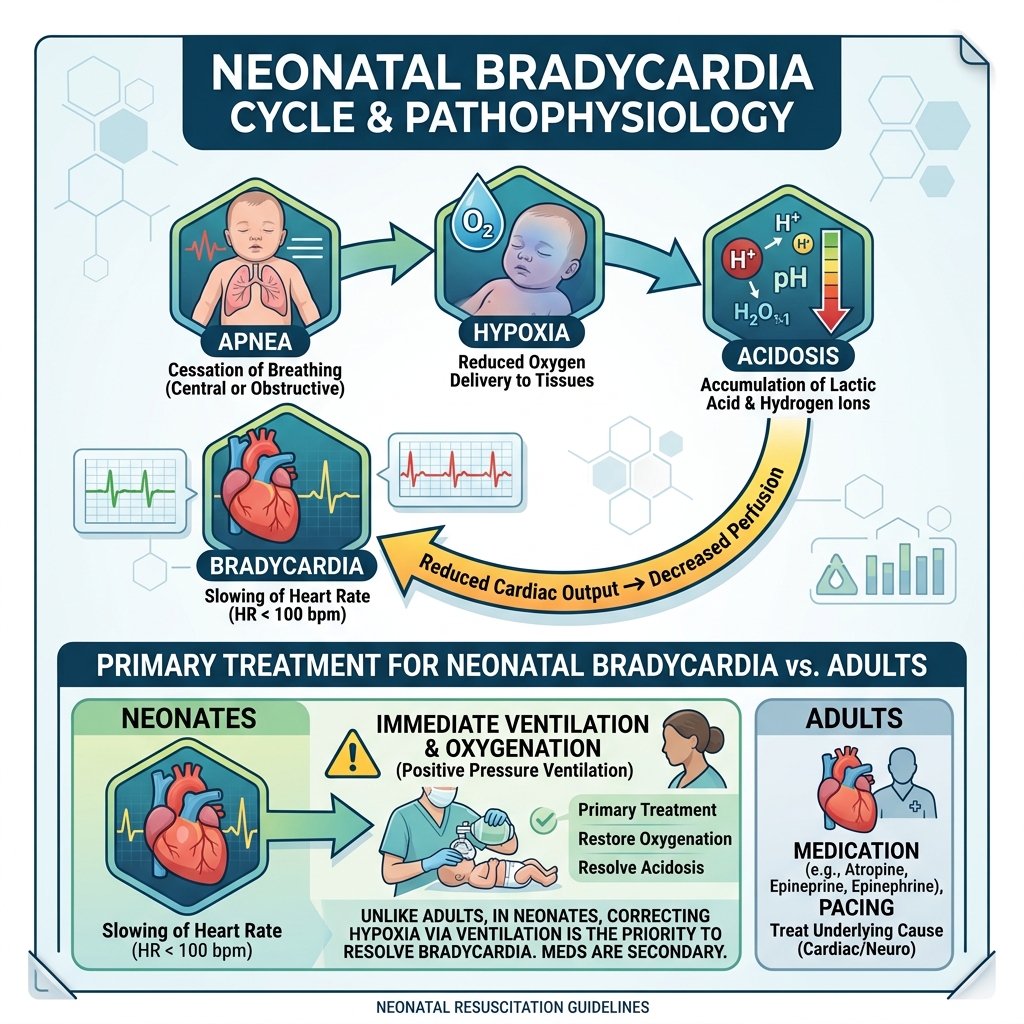
Neonatal bradycardia is most often a downstream effect of apnea, hypoxia, and rising CO₂ (hypercapnia) leading to acidosis.
Relationship to apnea
Key concept
Apnea → hypoxia → acidosis → bradycardia
- Bradycardia then worsens perfusion → more hypoxia
- → This creates a self-perpetuating cycle that must be interrupted early
Most common cause
Prematurity with an immature brainstem respiratory drive
Definition and clinical significance
Definition
- Technically: heart rate below age-based normal
- In practice: heart rate < 100 bpm
Clinical significance
- Bradycardia itself is rarely the primary problem
- It is usually a marker of inadequate oxygenation and ventilation
Critical takeaway
- Correcting hypoxia rapidly often reverses bradycardia
- Delays lead to worsening acidosis and deterioration
Other causes and risk factors
Other causes (less common)
- Increased intracranial pressure
- Hypothyroidism
- Congenital heart block (e.g., maternal autoimmune disease)
Clinical insight
If bradycardia occurs without apnea or hypoxia, consider non-respiratory causes
Risk factors
Vagal stimulation
Can trigger sudden bradycardia due to:
- Aggressive or prolonged suctioning
- Endotracheal tube manipulation
- Poor synchronization with assisted ventilation
Important concept
- Neonates are highly sensitive to vagal reflexes
- Over-intervention can worsen the situation
Management approach
Priorities: airway → breathing → circulation
Airway
Assess for:
- • Secretions
- • Tongue obstruction
- • Improper positioning
- • Foreign material
Key action
Clear airway if needed, but avoid excessive suctioning
Breathing
Evaluate for:
- • Hypoventilation
- • Apnea
- • Poor respiratory effort
Interventions
- Provide positive pressure ventilation (PPV) with oxygen
- Ensure visible chest rise
Escalation
Consider intubation if:
- Ventilation is ineffective
- Apnea persists
- Prolonged support is expected
Circulation
Assessment
Check heart rate via:
- Umbilical stump
- Brachial pulse
Treatment thresholds
- HR < 100 bpm
- Begin assisted ventilation with oxygen
- Reassess
- HR < 60 bpm
- Start chest compressions
- Continue ventilation
- HR 60–80 bpm and not improving
- Initiate compressions
Stop compressions when
Heart rate ≥ 100 bpm
Medications
Consider:
- Oxygen (primary therapy)
- Epinephrine if bradycardia persists despite adequate ventilation and compressions
Supportive care
- Maintain normal body temperature
- Optimize positioning
- Minimize unnecessary stimulation
Clinical patterns to recognize
Typical presentation
Bradycardia + apnea + hypoxia (especially in preterm infants)
Atypical presentation
Bradycardia without respiratory compromise
→ Think cardiac or neurologic causes
Transport
Early transport to a facility capable of neonatal critical care
Communication
- Clearly explain interventions to caregivers
- Emphasize that rapid treatment significantly improves outcomes
• Key concepts to lock in
- → Heart rate < 100 bpm = abnormal
- → Most cases are due to hypoxia from apnea
- → Ventilation is the priority intervention
- → Bradycardia is usually secondary, not primary
- → Start compressions if HR < 60 bpm
- → Avoid excessive suctioning (can worsen bradycardia)
- → Fix oxygenation → heart rate improves