LessonArtificial Ventilation and Capnography
Artificial Ventilation and Capnography
When providing assisted ventilations, the goal is not just to move air into the lungs—but to ensure that gas exchange is actually occurring at the alveolar level.
Limitations of Common Assessment Tools
Chest rise:
Confirms air entry, not effective gas exchange.
Pulse oximetry:
Reflects oxygenation, but responds slowly and may lag behind clinical changes.
Because of this, capnography is the most reliable real-time tool for evaluating ventilation.
What is Capnography?
Capnography measures carbon dioxide (CO₂) in exhaled air, specifically end-tidal CO₂ (ETCO₂).
CO₂ is only present if:
- Blood is delivering CO₂ to the lungs (perfusion)
- Air is reaching the alveoli (ventilation)
Ventilation Workflows
Patients Without an Advanced Airway
Initial Management
- Apply high-flow oxygen (NRB) while preparing for ventilation
- Position the patient supine (maintain spinal precautions if needed)
- Open and clear the airway
- Insert an airway adjunct (OPA/NPA) if indicated
Ventilation Technique
- Use a BVM connected to oxygen
- Maintain a tight mask seal
- Deliver each breath over ~1 second
Watch for: Visible chest rise, full exhalation between breaths
Ventilation Rates
Adults: 1 breath every 5–6 seconds (10–12/min)
Children: 1 breath every 3–5 seconds (16–20/min)
Infants: 1 breath every 2–3 seconds (20–30/min)
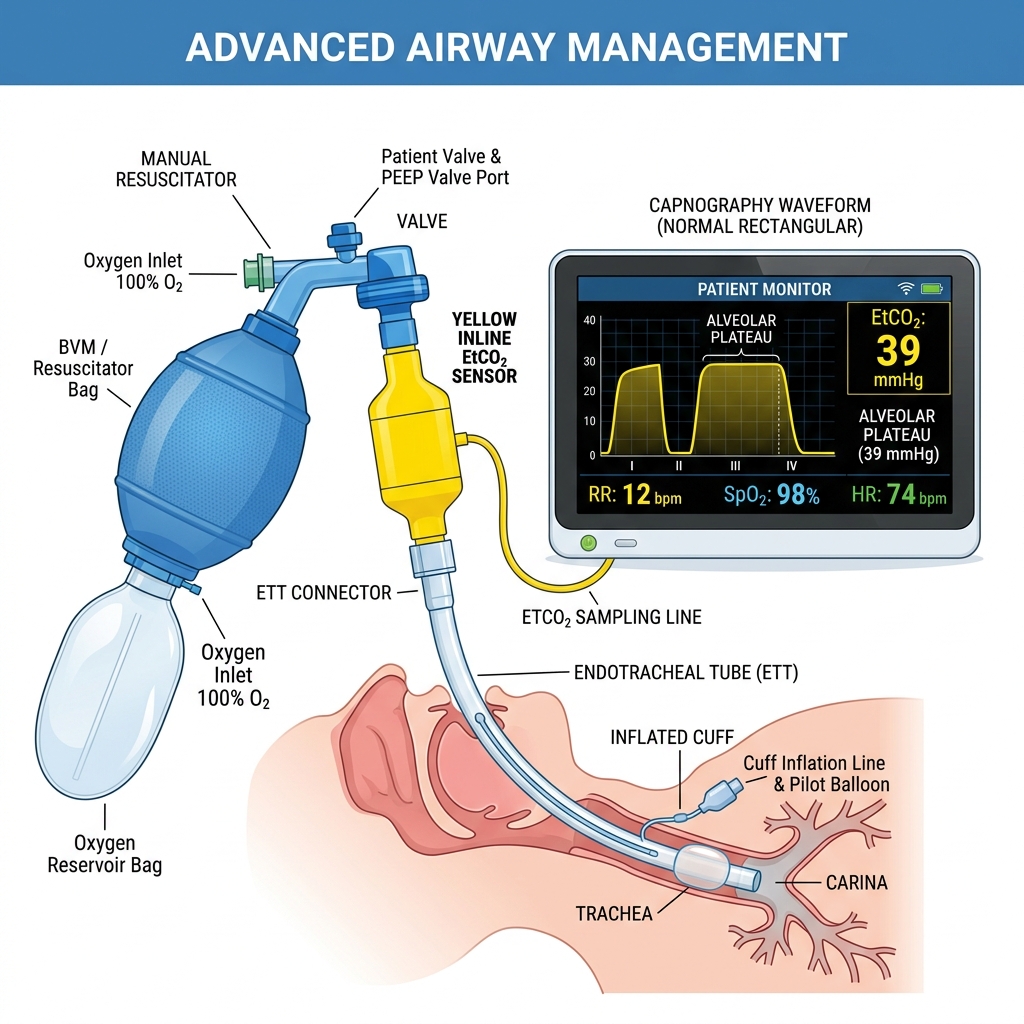
Patients With an Advanced Airway
(Intubated or has a tracheostomy)
Setup & Technique
- Connect ventilation device to oxygen
- Place inline capnography between airway and BVM/ventilator
- Deliver 1 breath every 6–8 seconds (8–10/min)
- Ensure equal chest rise and full exhalation
Confirming Airway Placement
Gas exchange only occurs in the lungs—not the esophagus.
If CO₂ detected → airway is in lungs
If CO₂ absent → suspect esophageal placement
Capnography & Monitoring
Colorimetric CO₂ Detection
Uses a chemical indicator that changes color when exposed to CO₂.
Typical change:
Limitation: Only confirms presence of CO₂, not trends or ventilation quality.
Capnometry vs Capnography
Capnometry
Provides a numeric or color-based reading.
Answers: "Is CO₂ present?"
Capnography
Provides a continuous waveform + numeric value.
- Ventilation effectiveness
- CO₂ production
- Airway integrity
Clinical Takeaways
- Effective ventilation = air movement + gas exchange
- Capnography is the gold standard for monitoring ventilation
- No CO₂ = no effective ventilation or wrong tube placement
- Pulse ox alone is too delayed to guide immediate decisions
- Always monitor ETCO₂ trends, not just a single value