LessonAngina & Acute Coronary Syndromes
Angina & Acute Coronary Syndromes
Chest pain related to the heart typically results from reduced blood flow to the myocardium. This exists on a spectrum ranging from temporary ischemia to irreversible tissue death.
Spectrum of Ischemic Chest Pain
Stable Angina
Predictable pattern.
Caused by temporary, partial reduction in coronary blood flow.
- Triggered by exertion or stress
- Gradual onset
- Described as pressure, tightness, or squeezing
- Lasts a few minutes (< 5 mins)
- Relieved by rest or nitroglycerin
Unstable Angina (ACS)
No longer predictable. Indicates worsening coronary perfusion.
- Occurs at rest or minimal activity
- Increasing frequency or severity
- Not reliably relieved by rest or nitro
Myocardial Infarction (Heart Attack): Prolonged ischemia leading to cell death. Most dangerous stage.
Causes of Angina / ACS
- Atherosclerosis: Plaque buildup narrows coronary arteries
- Coronary Vasospasm: Temporary vessel constriction (triggers include cold exposure, stress, smoking, cocaine, certain medications)
Progression Pattern
Chest pain may evolve as follows: Initial episode → Increasing frequency/duration → Pain at rest (pre-infarction) → Infarction.
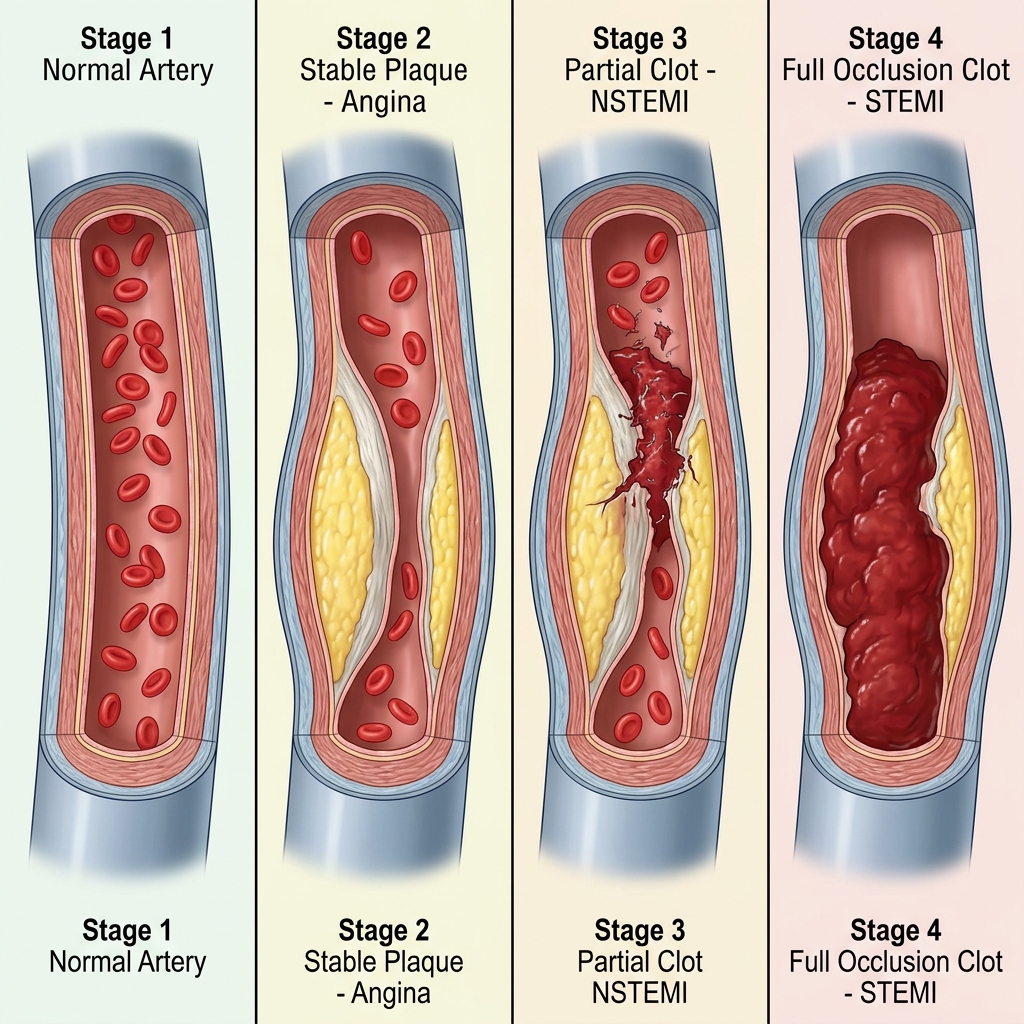
Classic progression: Stable angina → Unstable angina → NSTEMI → STEMI
Types of ACS
- Unstable Angina (UA): Ischemia without measurable heart muscle damage. No troponin elevation.
- NSTEMI: Myocardial damage present. May show ST depression or subtle ECG changes. Troponin elevated.
- STEMI: Full-thickness myocardial injury. ST elevation on ECG. Requires immediate reperfusion.
Troponin Role
Marker of myocardial injury. May not elevate for several hours.
In the field: UA and NSTEMI may appear identical.
Recognizing Ischemic Chest Pain
Typical cardiac pain: Pressure, squeezing, heaviness. Diffuse. May radiate to Jaw, Neck, Arm. Associated with Shortness of breath, Nausea, Sweating.
Non-Cardiac Chest Pain Clues: Less likely cardiac if the pain is sharp/stabbing with breathing, reproducible with palpation, localized with one finger, lasts seconds or is constant for days, or radiates to head/legs.
Field Approach
Without lab testing, focus on identifying likely ischemic pain.
- Aspirin (324 mg, chewable) - Reduces mortality
- Maintain Airway, Breathing, Circulation
- Position Upright if stable
- Oxygen Only if SpO&sub2; < 90%
- 12-lead ECG - Early acquisition is critical
- Nitroglycerin - If indicated and no contraindications
Key Takeaways
- Cardiac chest pain exists on a progressive spectrum
- Stable angina becomes dangerous when it loses predictability
- UA, NSTEMI, and STEMI are often indistinguishable early
- Always assume ischemia if unsure
- Early aspirin and ECG are critical interventions