LessonNeurogenic Shock
Neurogenic Shock
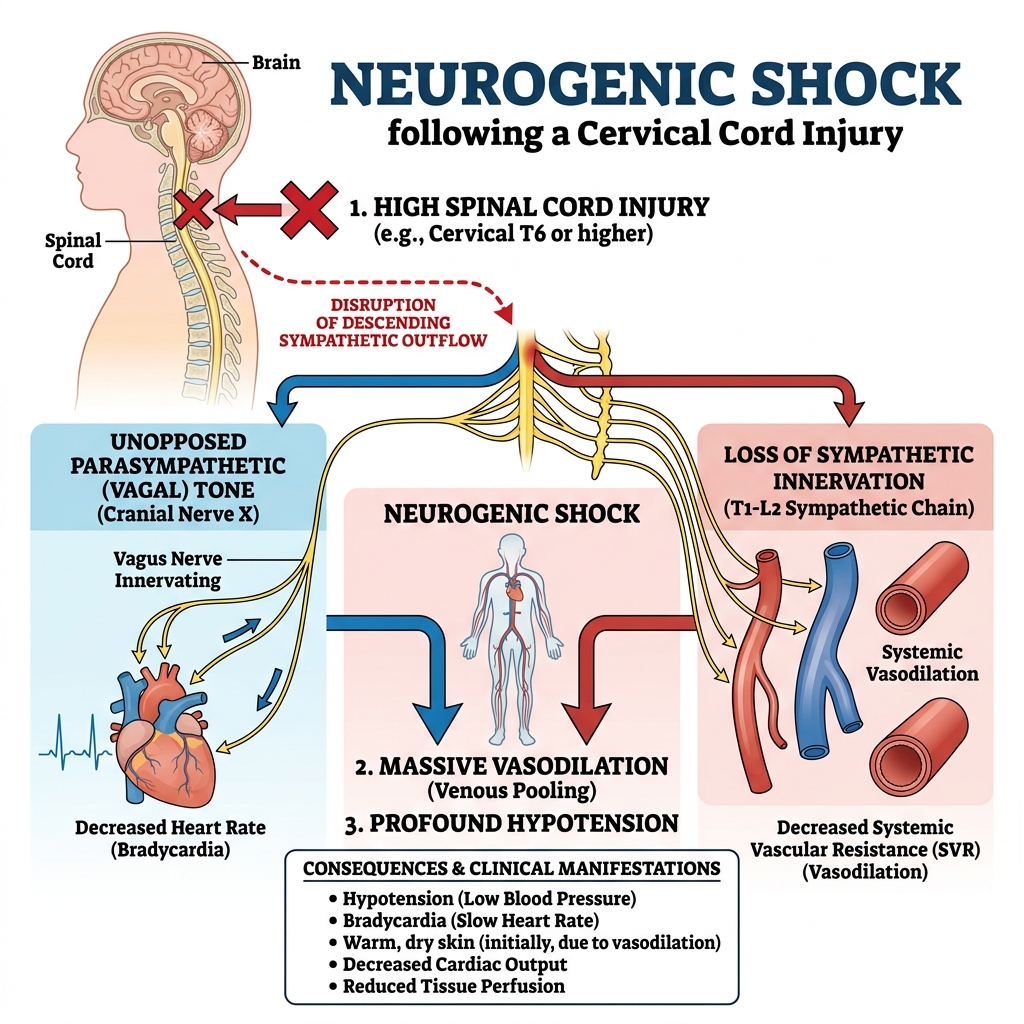
Neurogenic shock is a form of distributive shock characterized by widespread vasodilation due to disruption of the autonomic nervous system. This leads to decreased vascular tone, reduced systemic vascular resistance, and impaired perfusion.
It most commonly occurs following a spinal cord injury, particularly when the sympathetic pathways are affected.
Pathophysiology
Normal cardiovascular function depends on a balance between Sympathetic tone (increases heart rate and vasoconstriction) and Parasympathetic tone (vagus nerve, slows heart rate).
In neurogenic shock:
- Injury to the spinal cord disrupts sympathetic outflow.
- The parasympathetic system becomes unopposed.
Vasodilation
→ Decreased SVR
Bradycardia
→ Reduced cardiac output
Hypotension
→ Inadequate tissue perfusion
Clinical Presentation
Key Findings
- Hypotension
- Bradycardia (The hallmark combination!)
- Warm, flushed skin (due to vasodilation)
- Altered mental status (decreased cerebral perfusion)
- Motor deficits/paralysis (depending on injury level)
Concurrent Hemorrhage
Patients with spinal trauma may also have concurrent hemorrhage.
→ Hypotension may be multifactorial. Always consider hypovolemic shock as a coexisting condition.
Prehospital Management
Immediate spinal immobilization to prevent further neurologic injury.
Initiate IV/IO access. Administer fluids to support perfusion (Goal: Maintain adequate perfusion pressure, commonly targeting MAP ≥ 90 mmHg).
Often required due to loss of vascular tone. Norepinephrine is commonly used to restore vascular resistance.
Atropine may be used for symptomatic bradycardia.
Clinical Pearl
If a trauma patient presents with hypotension AND bradycardia, think neurogenic shock—but always rule out hemorrhage first.